You will find that in the long version, each statement is very well documented. If you disagree with something I've written, please take the time to read the quotes provided before returning to Colbert's Vax-Scene. If that can't help you understand what was done to you, nothing can...
There are many subjects to cover, and I leave no stone unturned. When you get to the end of this article, if you take the time to read the citations, you will have a better understanding of relevant aspects of immunology, microbiology, virology, pathology and proteomics than the vast majority of physicians. You already know some of them, but many are new. What you do with this information is up to you, but I ask that you use it to help people in need. After they apologize, maybe. Clott Adams, lead the way!
Without further ado, let's get to the heart of the matter.
A brief outline of everythingThe immune system is generally considered to consist of two major domains: innate and adaptive.
For the purposes of this article, I expand it to four: innate, adaptive, complementary, and cytosolic. In this way, we will be able to identify, compare, contrast, characterize and explore more precisely the relevant aspects of each of them. This will not be a complete presentation; I could spend a lifetime trying to write it. I will instead focus on the relevant sections and discuss them.
Adaptive Immunity: AntibodiesAdaptive immunity is, to a large extent, centered on the recognition of antigenic peptides, the production of antibodies, the subsequent binding of these antibodies to pathogens, and the interaction of these bound antibodies with various immune cells to trigger various functions. . There are several classes and several subclasses. The ones we are going to focus on are the IgG class antibodies.
de Taeye, SW, Rispens, T., & Vidarsson, G. (2019). Human IgG ligands and their effector functions. Antibodies, 8(2), 30.
https://doi.org/10.3390/antib8020030Upon naïve exposure to a given pathogen, the first antibodies to be deployed will be those of the IgM class. They are very broad and nonspecific, and constitute the first step in building immunity against a given pathogen: once the infection has progressed, pathogen-specific IgG antibodies begin to form. IgG1, IgG2 and IgG3 all play crucial, sometimes overlapping roles: after binding to the pathogen, they activate the complement system, mark pathogens for phagocytosis by innate and adaptive immune cells, neutralize virus entry proteins, transport bound proteins to lymph nodes for examination, etc.
IgG4 is the ANTI-antibody. It does not neutralize pathogens, target them, or activate complement: rather, it signals to anything it encounters that its prey is harmless and should not be attacked. IgG4 is expressed upon repeated exposure to a foreign body that dendritic cells, the masterminds of the immune response, have determined to be harmless. The main example of their function is to prevent unnecessary immune response to pollen. Although they have been implicated in autoimmune diseases, this is not the subject that interests us here. I continue the army analogy: IgG4 is a flashing IFF (Identification Friend or Foe) signal.
An IgG4 response to a dangerous replicating pathogen is probably the worst response we could have induced, and as we noted at the start, that is exactly what happens. Serum levels of different IgG subclasses normally vary somewhat in response to infection.
What is not normal is the fact that a few months after a booster - we do not know exactly how many, which may also reflect the fact that the vast majority of vaccines administered are probably more or less inactive - the rates levels of IgG1, IgG2 and IgG3 fall sharply and the response is dominated by IgG4!

- IMG_20230129_063306.png (99.01 KiB) Viewed 1194 times
Irrgang, P., Gerling, J., Kocher, K., Lapuente, D., Steininger, P. et al. (2022). Class switch towards non-inflammatory, spike-specific IgG4 antibodies after repeated SARS-COV-2 mRNA vaccination. Science Immunology.
https://doi.org/10.1126/sciimmunol.ade2798There are several dangerous pitfalls that should have been considered in the process of testing these vaccines. The main point of alarm for immunologists has, until now, been the original antigenic sin: if the immune response is highly trained to recognize only one pathogen-specific peptide, when it encounters a mutated version , incorrectly shaped, non-binding, non-neutralizing antibodies will be produced, and the pathogen will have much more freedom to reproduce and cause disease until the rest of the immune system catches up. In animal trials, death occurs very frequently before this time. Coronaviruses, in particular, were thought to be particularly susceptible to this problem, due to extensive animal trials in the 2000s, with vaccines tested against previous incarnations of SARS, in which all vaccinated animals routinely died. . [Note Obamot: Pfizer would not have included animal testing, as all would have died]
Original antigenic sin has proven, over time, to be less of a concern than previously thought, with most vaccinated people still able to mount an immune response despite defective and outdated mRNA proteins. This must be said, of course, with the major caveat that we don't actually know what proportion of the vaccines are actually active and producing the peak as expected. Adverse event rates are very strongly correlated to specific lots, so it is very reasonable to assume that they are not all the same. The silver lining for those who didn't get a "hot shot" is that you might not have to worry about any of that. Check your lot number here [for all links, see V/en.
The real concern now is the unexpected shift to IgG4, and therefore immune tolerance. I will detail this point after covering the other relevant aspects of the immune system.
Adaptive immunity: T lymphocytesT cells are the big shots of the adaptive immune system. There are two main classes: CD4 and CD8.
CD4 helper T cells act as the colonels of the battlefield, activating, directing and deactivating the responses of other cells by releasing various cytokines, and receiving orders from HQ. Their depletion is a hallmark of advanced HIV/AIDS; with limited or absent CD4 activity, the immune response is severely blunted and lymphocyte recruitment to the site of infection is reduced. CD4 is already somewhat depleted even during normal SARS-CoV-2 infection, due to spike protein HIV gp-120 homologous regions that exert a pyroptotic effect on CD4 through interaction with CD4/CCR5 receptors. It has also been observed to directly infect CD4 T cells, much like – you guessed it – HIV.
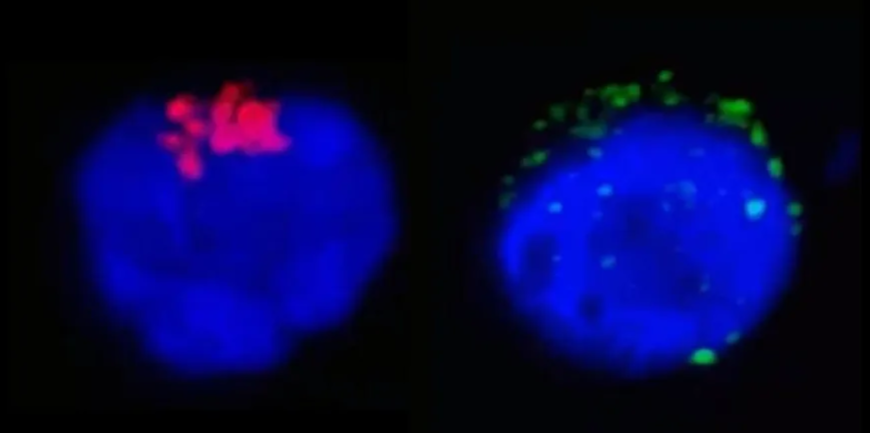
- IMG_20230129_063842.png (163.99 KiB) Viewed 1194 times
CD4+ T cell infected with SARS-CoV-2, showing RdRp (left) and Spike (right). Brunetti, NS, Davanzo, GG, de Moraes, D., et al. (2020). SARS-COV-2 uses CD4 to infect helper T cells.
https://doi.org/10.1101/2020.09.25.20200329Continuing the battlefield analogy: If CD4s are the colonels, CD8 cytotoxic effector T cells could be the air support. After activation by CD4 cytokines, subsequent recognition of an antigen on the cell surface in the MHC-I complex, and CD28, CD80 and CD86 cytokines on the surface of an infected cell, CD8 begin to attack the infected cell with perforins and granzymes to destroy it. CD8 is unique in that it is able to target cells, such as neurons and gonadal cells, that are otherwise privileged against immune attack; given the wide variety of cells that SARS-CoV-2 is able to infect, this is a saving grace that allows us to eliminate what would otherwise have become a very difficult latent chronic infection. CD8 is one of our immune system's most powerful weapons, although it can also cause significant collateral damage to uninfected tissue.
Innate Immunity: Phagocytic CellsInnate immunity is made up of the immune cells which, in a very general way, act not on the recognition of particular antigens, but on immune signals, called cytokines, which are released by all kinds of cells for a wide variety of purposes. . In response to various cytokines, innate immune cells can become active or inactive, be produced in greater or lesser numbers, use chemotaxis to migrate to a site of infection, and release their own cytokines to coordinate with the broader immune system .
The innate immune cells of interest here are neutrophils, monocytes, macrophages and dendritic cells.

- 96f11de8-f40c-4838-8679-bd4a6e07295d_400x300.gif (7.16 Mio) Consulté 1194 fois
Gluttonous phagocytosis.
Neutrophils are the very first innate line of defense and are perhaps the most effective countermeasure we have against SARS-CoV-2. Faced with the class change of IgG4, they are probably the only defense that retains useful functionality. Neutrophils are the only ones that do not interact significantly with IgG4: if they encounter an infected cell or a free virion, they destroy or consume it, respectively, and release cytokines to promote inflammation and the immune response. . They are, however, a double-edged sword: thanks to a quirk in our evolution, we lack a crucial component necessary for them to function properly, which we can now only obtain from our diet; without sufficient amounts of this component, which is never present without very deliberate and well-informed administration, neutrophils become rapidly depleted upon deployment and undergo NETosis, a unique form of apoptosis by which proteins in the form of net are released to trap any nearby pathogens and strongly promote local inflammation. (Their non-interaction with IgG4 is a saving grace that, if properly applied, can save lives,) even if the immune response is otherwise completely shut down.
Monocytes and macrophages are important both for the direct destruction of infected cells, the phagocytosis of free virions, the presentation of viral peptides to dendritic cells for their recognition and the production of antibodies, and the signaling of cytokines to cause a localized inflammation and greater immune involvement. I won't go into them in detail here – you'll find out why in a moment – but each of these functions is vitally important to the success of the immune response to SARS-CoV-2 infection.
Dendritic cells are the brains of the adaptive immune system. By capturing the freely soluble antigenic peptides in serum, usually present due to CD8 destruction of an infected cell, they assess the antigen and determine the appropriate immune response. If the CD4 T cells are the colonels who direct the battle, the dendritic cells are the generals who direct the war, and the CD4, CD8, B cells and others receive their instructions from the dendritic cells. They are responsible for directing the class change to IgG4; the whys and wherefores are not particularly well understood, nor particularly relevant at this time, to a vaccinated person's ability to survive infection. For the same reason, I will not discuss them in detail.
Complement: Rube Goldberg's MachineIf we have discussed the generals and colonels of this war, the complementary immune system can be described as roaming bands of hostile neighborhood children: they summon the adults, leave grenades in your path, shoot you and, occasionally, cause trouble for no reason.
Complement is a fabulously complex system of interconnected proteins, ubiquitous in bodily fluids. They work through signaling pathways and cascading interactions; upon detection of a pathogen, or sometimes completely randomly, they begin what is known as a complementary cascade, gradually binding to each other, as well as to various immune cell receptors, in order to alert the immune system to a potential problem. The complementary immunity cascade is a vital part of any immune response and contributes to both the activation of the immune system and the localization of immune cells to an area of infection. Their communication is two-way: the wider immune system can also inactivate the cascade, usually upon resolution of the infection, when an immune response is no longer needed.
I will not expand further on complementary immunity.
Are you starting to wonder why?
Cytosolic immunity: Rube Goldberg's other machineCytosolic functions relating to the immune system are generally classified under the category of innate immunity. However, for the purposes of this article, I consider them a class apart, and I generally refer to non-immune cells: endothelial cells, myocytes, parenchymal cells, and neurons, to name a few. The cellular cytosol is the interior of any given cell, excluding the interior of organelles such as mitochondria, inside which most of the cellular processes essential for life take place. Many functions carried out inside the cell are linked to the proper functioning of innate and adaptive immunity in the broad sense, within which there are defense mechanisms against infections that do not require any external intervention. Like complement, they act in cascade and depend on many interactions. The most relevant functions are the NF-κB pathway, Toll-like receptors and major histocompatibility complex I (MHC-I). There are, broadly, three distinct signaling cascades that occur upon viral infection of a cell.
The first is the most optimal. If the cell has already been warned of a potential infection by the release of interferons from neighboring cells, it will be primed for infection; TLR3, TLR7 and RIG-I will detect the viral particle in the endosome, endosomal maturation will occur and transform it into endolysosome, which will proceed to destroy the viral protein; and the cut peptides will be presented at the cell surface in an MHC-I protein complex, to be presented to the adaptive immune system. The cell will also release interferons to warn neighboring cells again.
The second case is the most common. If the cell is unprepared for infection, the immune avoidance functions of SARS-CoV-2 allow it to prevent both endosomal maturation and detection, thus allowing endosomal escape of the viral protein in the cell, where it begins to replicate; other immune avoidance functions interfere with the production of MHC-I and interferons, allowing the infection to go undetected by the general immune system for a time, but not indefinitely, and the cell then releases interferons to warn neighboring cells. This describes the initial stages of most naïve infections.
The third stage is the one that our unfortunate vaccinated will undergo. In a process similar to antibody-dependent boosting, binding of the IgG4 antibody allows viral endocytosis via cell surface Fc receptors, as opposed to the more common ACE2 receptor. The binding of the FcγRIIB receptor by the IgG4-virion complex leads to the binding of PI3K to the nuclear localization signal of the NF-κB factor,
which inhibits the production of cytokine signals and MHC-I surface presentation of viral peptides. In concert with the immune evasion functions of SARS-CoV-2,
this allows the virus to replicate completely unchallenged and undetected by the immune system.
SynthesisIf you've made it this far, congratulations! We covered the basics of immunology that apply to SARS-CoV-2 infection. In summary, the most relevant and necessary immunological functions to respond to SARS-CoV-2 infection are:
— Dendritic cells: Recognition of viral peptides, determination of the class of immunoglobulins (antibodies) to be produced; cytokine signaling to activate immune responses. (Generals)
“B-cells are gunsmiths, but they're largely irrelevant to this discussion.
— CD4 T cells: Recognition of the viral antigen, dendritic signalling, command and control (C&C) of the local immune response. (Colonels)
— Neutrophils: Phagocytosis of free virions, attack of infected cells, and cytokine signaling: powerful, but in most circumstances very limited, and a double-edged sword. (Heavy armor)
_ Monocytes and macrophages: As above, and presentation of viral peptides to the various C&C cells. (Light Armor)
— CD8 T cells: Destruction of infected cells. (Air Support)
— Antibodies: Neutralization of virus entry proteins, and binding to virions to facilitate phagocytosis - or in the case of IgG4, shutting down almost the entire immune response. (Infantry)
— Complementary immunity: Initial and ongoing detection and signaling of viral infection, and localization of infection to facilitate immune cell chemotaxis. (Civilians)
— Cytosolic functions: Detection of viral infection, surface presentation of viral peptides to the adaptive immune system, release of interferons and cytokines to activate the immune response. (civil infrastructure)
________________________________
It's awesome"! Everything a well-rounded immune response needs to get you through a war with COVID, all in one tidy, human-shaped package.
Here's what you get when your adaptive immune response is heavily dominated by, or exclusively composed of, IgG4 antibodies.
Shit. Neutrophils.

- IMG_20230129_070044.png (573.45 KiB) Viewed 1194 times
You didn't havedon't really need that immune system";in any event.I hope you now have an idea of how insanely bad it is.Final sarcastic noteOf course, you didn't read any of the quotes, so in fact, the only evidence I gave you for that statement was an old South Park meme. Why should you believe me? You shouldn't, of course. I'm a far right anti-vaxx who thinks he's a horse, and probably also a bigoted racist transphobe, right? That's why I'm going to show you the proteomics of each interaction that causes it. There must be absolutely no debate about this: it is real, it is, and as surely as we can see that yin adapts to yang, we can see that an IgG4-dominated response to SARS-CoV-2 is a total and unprecedented disaster that is slowly brewing among billions of people on the planet.


